





Sepsis affects millions worldwide and is responsible for roughly 20% of global deaths. Traditionally, it was thought that sepsis-related mortality was due primarily to an excessive inflammatory response that damages vital organs such as the lungs and kidneys. However, growing evidence shows that immune suppression—also known as immune paralysis—can be equally deadly.
In this state, the immune system is no longer able to mount an effective defence. Patients become highly susceptible to secondary infections, particularly from fungi and drug-resistant bacteria, complicating their already critical condition.
When the immune system falters, the body becomes vulnerable to infections that would otherwise be kept in check. In the case of sepsis—a life-threatening condition marked by an imbalanced immune response to infection—this dysfunction can be deadly. Researchers have identified a promising way to restore immune function using a drug already approved for another condition (Figure 1). Their findings offer a potential path forward for treating patients in intensive care units (ICUs), where sepsis remains a leading cause of mortality.
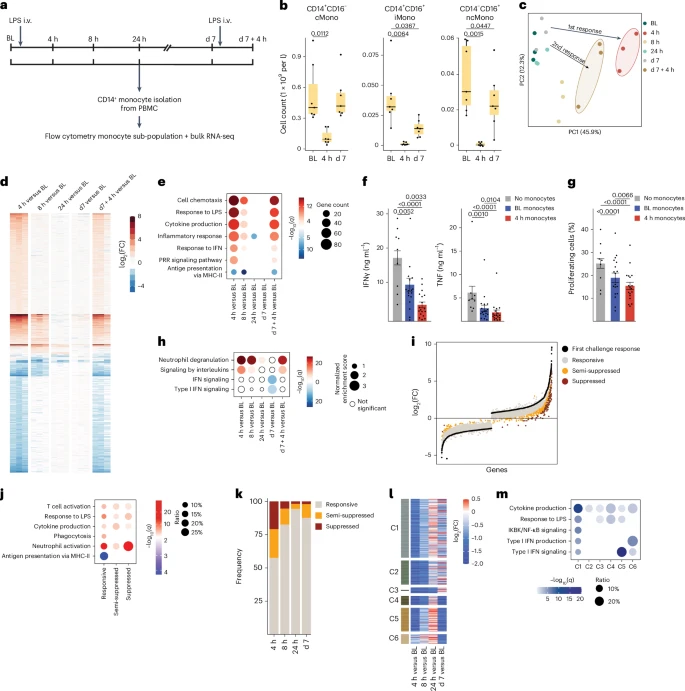
Figure 1: Impairment of IFN-I pathway in blood monocytes 1 week after LPS-induced systemic inflammation. a, Schematic representation of the study and sample acquisition in healthy volunteers (n = 11). Seven volunteers were intravenously (i.v.) injected with LPS (2 ng kg−1) at baseline (BL, d0) and d7. Four volunteers were intravenously injected with placebo (0.9% NaCl) at BL. Peripheral blood was collected at BL, 4 h, 8 h, 24 h, d7 and d7 + 4 h. b, Box plots of absolute abundance of CD14+CD16− cMonos, CD14+CD16+ iMonos and CD14−CD16+ ncMonos in blood of LPS-challenged volunteers (n = 7) at BL, 4 h and d7. c, Principal component analysis of blood CD14+ monocyte transcriptomes from LPS-challenged volunteers (n = 3) at BL, 4 h, 8 h, 24 h, d7 and d7 + 4 h. d, Heatmap representation of DEGs at 4 h, 8 h, 24 h, d7 and d7 + 4 h compared with BL as in c. e, GO term analysis of DEGs at 4 h, 8 h, 24 h, d7 and d7 + 4 h compared with BL as in c. f, Bar plots of TNF and IFNγ production in CD3+ T cells isolated from the blood of healthy donors (n = 9), activated with CD3 and CD28 antibody-coupled beads and co-cultured with cMonos obtained from LPS-challenged volunteers (n = 6) at BL and 4 h at 1:2 ratio. g, Bar plots of percentage of proliferating CD3- and CD28-activated CD3+ T cells isolated from the blood of healthy donors (n = 9), and co-cultured with cMonos obtained from LPS-challenged volunteers (n = 6) at BL and 4 h at 1:2 ratio as in f. h, GSEA of gene expression profiles at 4 h, 8 h, 24 h, d7 and d7 + 4 h compared with BL as in c. i, DEGs in blood CD14+ monocytes from LPS-challenged volunteers (n = 3) in response to both LPS challenges (first: 4 h versus BL; second: 7 d + 4 h versus 7 d) clustered into three groups: responsive (FC < 2), semi-suppressed (2 < FC < 3) and suppressed (FC > 3). j, GO term analysis of responsive, semi-suppressed and suppressed genes in CD14+ monocytes from LPS-challenged volunteers (n = 3) as in j. k, Percentage of responsive (FC < 2), semi-suppressed (2 < FC < 3) and suppressed (FC > 3) DEGs in blood CD14+ monocytes from LPS-challenged volunteers (n = 3) obtained at 4 h, 8 h, 24 h and d7 that were ex vivo stimulated with LPS (10 ng ml−1) versus CD14+ LPS-stimulated monocytes obtained at BL. l, Heatmap representation of average expression of DEGs in CD14+ restimulated monocytes from LPS-challenged volunteers (n = 3) obtained at 4 h, 8 h, 24 h and d7 based on fold-change relative to BL (n = 3) as in k. Genes were clustered (C1–C6) based on their behavior across the different time points. m, GO term analysis of genes in clusters C1–C6 defined as in l. The box plots in b show the median, first and third quartiles and the whiskers 1.5× the interquartile range (IQR). The bar plots in f and g are presented as mean values ± s.e.m. The P values were calculated using two-sided, paired Wilcoxon’s signed-rank tests.
To better understand how immune paralysis develops, the team conducted controlled studies in healthy volunteers. By administering endotoxins—harmless fragments of bacterial cell walls—they triggered a temporary immune response and followed its progression using cutting-edge immunological tools.
In samples taken from participants’ blood and bone marrow, they observed that monocytes, failed to mature properly after the initial immune activation. These dysfunctional cells were less effective at defending against infection, shedding light on one of the mechanisms driving immune paralysis.
The researchers next tested whether interferon beta—a drug commonly used to treat multiple sclerosis—could restore function to these impaired immune cells. In lab experiments, adding interferon beta to paralyzed monocytes prompted them to mature and regain their infection-fighting capabilities.
While the results are promising, more research is needed before the approach can be tested in patients with sepsis. Future studies may also explore whether the treatment can improve monocyte function directly in ICU patients with sepsis. If successful, this could mark a significant advance in managing a condition that remains notoriously difficult to treat.
Journal article: Keramati, F., et al., 2025. Systemic inflammation impairs myelopoiesis and interferon type I responses in humans. Nature Immunology.
Summary by Stefan Botha



