





- Patient Presentation
- History
- Differential Diagnosis
- Examination (18 hrs post injury)
- Examination (3 wks post injury and eye repair)
- Investigations
- Discussion
- Treatment
- Final Outcome
- References
- Evaluation - Questions & answers
- MCQ
Patient Presentation
A 12 year old boy is brought into the paediatric casualty by his parents approximately 18 hours after sustaining a penetrating knife injury to his left eye.
Partnership
We have partnered with The International Union of Basic and Clinical Pharmacology (IUPHAR) to bring you in-depth information about drugs and pharmacology with links to the Guide to ImmunoPharmacology.
History
- The child was involved in a fight after school where he was attacked by a fellow learner who stabbed him in his left eye. He sustained no other injuries as his attacker ran away after the incident.
- The eye sustained minimal bleeding and although the boy was in some pain he insisted initially that he did not need any medical attention. The eye was cleaned and dressed at home.
- The next morning his eye was swollen shut with excessive bruising and pain. He was unable to open his eye. At this time his parents decided to bring him to the emergency room.
- He complained of headache which had started that morning and watering in the uninvolved right eye.
- No loss of consciousness or seizures had been noted since time of injury
Past Medical History
- Child had chicken pox at age 6 years, made a full recovery
- No other significant medical history
Past Surgical History
- Tonsillectomy at age 4, for recurrent episodes of tonsillitis
Family History
- Father is asthmatic, on treatment
- Mother is in good health
- One sibling aged 8 years, currently well
Allergies
- None known
Social History
- Lives with parents and sibling in a two bedroom apartment with electricity and running water.
Differential Diagnosis
- Trauma to left eye, right eye intact and uninvolved at time of injury
- Three weeks post injury- uveitis
- Sarcoidosis
- Syphilis
- Sympathetic ophthalmia
Examination (18 hrs post injury)
Initial Presentation, approximately 18 hours post injury
Appearance
- Well nourished child in obvious pain and discomfort. Left eye swollen shut with excessive periorbital bruising and swelling. No other injuries immediately apparent.
- GCS 15/15
- Awake, alert, and co operative
Vitals
- Temperature: 37.3°C
- Blood pressure 100/68
- Heart rate 75
- Respiratory rate 30
General
- No pallor or jaundice
- No signs of dehydration
- No lymphadenopathy
- No oedema
Head and Neck
Right Eye
- No abnormalities detected
- 20/20 visual acuity
- Visual fields, accommodation and light reflex intact
- Dilated retinal examination, no pathology noted
Left eye
- Excessive swelling and bruising
- On examination of eye, prolapse of the iris, ciliary body and retinal tissue noted
- Severely decreased visual acuity, complained of blurring, unable to assess with Snellen’s chart, only able to visualise fingers
- Dilated retinal examination not done at this time
Chest
- Trachea centrally located.
- Chest clear on auscultation
- No abnormalities detected
Cardiovascular
- No raised JVP
- Normally placed apex beat
- S1 and S2 heart sounds present, no murmurs.
- No abnormalities detected
Abdomen
- Not distended
- Soft and non tender
- Bowel sounds present
- No abnormalities detected
Neurological
- Higher function intact
- Normal level of consciousness
- Gait normal
- Power 5/5 globally
- Tone normal globally
- Reflexes 2/4 for both upper and lower limbs
Dermatological
- No rashes noted
Examination (3 wks post injury and eye repair)
Presentation, three weeks post injury and repair of left eye
Complaining of photophobia, bilateral eye pain, decreased vision and red eyes.
Appearance
- Child in severe pain and discomfort, assisted by parents as appears unable to open eyes.
- GCS 15/15
- Awake, alert, and co operative
Vitals
- Temperature: 38.0°C
- Blood pressure 120/74
- Heart rate 98
- Respiratory rate 35
General
- No pallor or jaundice
- No signs of dehydration
- Bilateral cervical lymphadenopathy
- No oedema
Head and Neck
Right Eye
- Red eye, tearing and photophobia
- On slit lamp examination large keratic precipitates and small depigmented nodules (Dalen-Fuchs nodules) seen on the retinal epithelium.
- Mild panuveitis (anterior and posterior chamber)
- Decreased visual acuity, 20/200
- Testing accommodation caused pain in the left eye
Left Eye
- Excessive swelling and pain
- Severe panuveitis
- Visual loss
Chest
- Trachea centrally located.
- Chest clear on auscultation
- No abnormalities detected
Cardiovascular
- No raised JVP
- Normally placed apex beat
- S1 and S2 heart sounds present, no murmurs.
- No abnormalities detected
Abdomen
- Not distended
- Soft and non tender
- Bowel sounds present
- No abnormalities detected
Neurological
- Higher function intact
- Normal level of consciousness
- Gait normal
- Power 5/5 globally
- Tone normal globally
- Reflexes 2/4 for both upper and lower limbs
Dermatological
- No rashes noted
Investigations
| Examination | Value | Normal Limits |
|---|---|---|
| Initial presentation | ||
| WBC | 11 | (4-12 x109/L) |
| HB | 13.1 | (12.1-15.2 g/L) |
| Platelets | 341 | (140-450 x109/L) |
| CRP | 35 | (0-8mg/l) |
| NA | 137 | (135-147 mmol/L) |
| K | 4.0999999999999996 | (3.3-5.0 mmol/L) |
| Cl | 101 | (99-103 µmol/L) |
| C02 | 18 | (18-29 mmol/L) |
| Urea | 4.2 | (2.5-6.4 mmol/L) |
| Creatinine | 65 | (62-115 mmol/L) |
| Corrected Calcium | 2.33 | (2.1-2.6mmol/l) |
| Phosphate | 1.04 | (1.0-1.5 mmol/l) |
| Magnesium | 0.86 | (0.8-1.3) |
| 3 weeks later | ||
| WBC | 16 | (4-12 x109/L) |
| HB | 12.1 | (12.1-15.2 g/L) |
| Platelets | 250 | (140-450 x109/L) |
| CRP | 85 | (0-8mg/l) |
| NA | 138 | (135-147 mmol/L) |
| K | 4.5 | (3.3-5.0 mmol/L) |
| Cl | 100 | (99-103 µmol/L) |
| C02 | 18 | (18-29 mmol/L) |
| Urea | 4.2 | (2.5-6.4 mmol/L) |
| Creatinine | 68 | (62-115 mmol/L) |
| CSF cell count | (0 cells) | |
| Polys | 0 | |
| lymphocytes | 0 | (0 cells) |
| erythrocytes | 15 | |
| Bacteria | No growth | |
| IgG | 5.8 | (4-10) |
| IgM | 1.01 | (0.5-2.2) |
| IgA | 0.6 | (0.5-2.2) |
| HIV Elisa | negative | |
| Blood Culture | negative |
Discussion
Sympathetic ophthalmia (SO) is a rare, bilateral, non-necrotizing, granulomatous uveitis that occurs after ocular trauma or surgical procedures to one eye threatening sight in the fellow eye. The pathophysiology is not clearly understood, but it appears that the disrupted integrity of the inciting eye leads to an autoimmune reaction against the exposed ocular antigens in the injured eye as well as in the sympathizing eye. In our case study the patient sustained a penetrating eye injury to his right eye which was surgically repaired within 24 hours and treated with topical and systemic steroids. The patient was however non compliant with treatment and three weeks later returned with bilateral panuveitis and loss of visual acuity.
With the aid of our full colour graphics this discussion aims to explain the pathophysiology behind sympathetic ophthalmia including an essential discussion of the immune tolerance mechanisms, which render the eye an immune privileged organ.
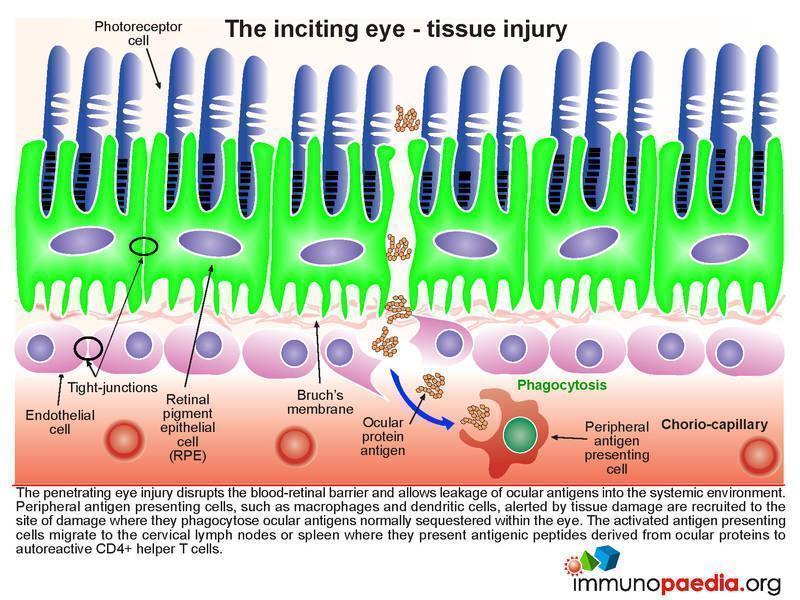
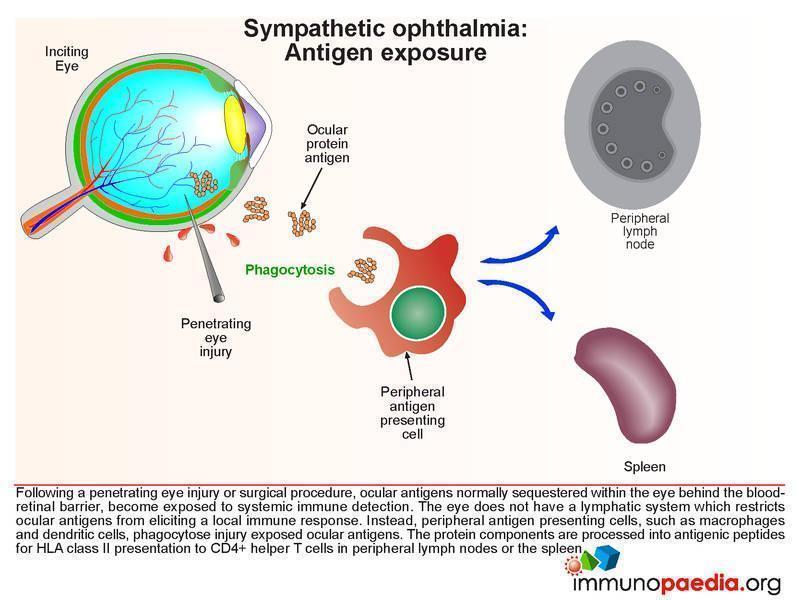
Antigen exposure and tissue injury
Ocular antigens are normally sequestered within the eye behind the blood-retinal barrier, thus preventing exposure of these antigens and their detection by the systemic immune system. However, in the event of a penetrating injury or surgical procedure this barrier is breached and ocular antigens leak into the systemic environment. The tissue damage alerts and recruits antigen presenting cells, such dendritic cells, to the site where they phagocytose and process the free ocular antigens into peptide fragments. CD4+ helper T cells recognize the peptides presented by class II HLA in distal secondary lymphoid structures, such as lymph nodes or the spleen.
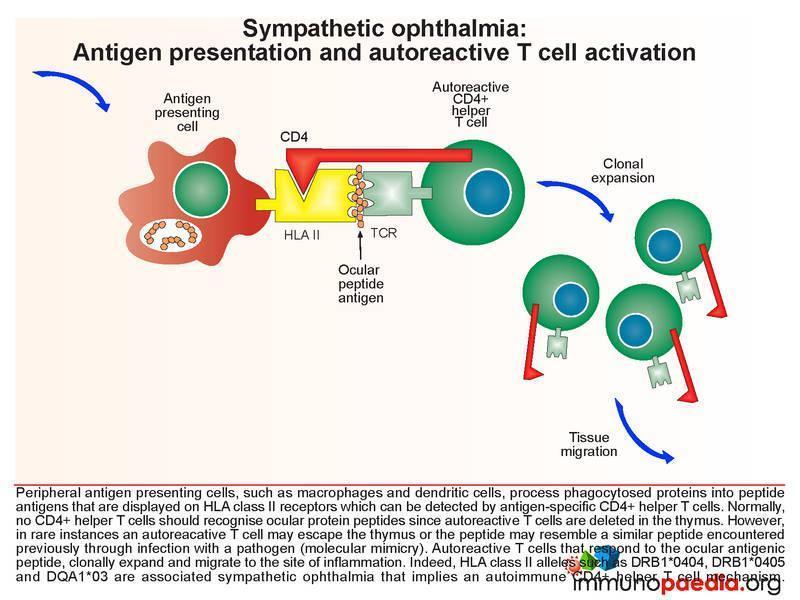 Under normal circumstances, where ocular antigens remain in the eye, CD4+ helper T cells do not recognise ocular proteins because autoreactive T cells are deleted in the thymus during T cell development. However, there are rare instances when an autoreactive T cell develops because there is cross-reactivity between the ocular peptide and a previously encountered peptide, which may have occurred in response to previous immune responses to other infections. This cross-reactivity with a peptide seen previously in an infection is known as molecular mimicry. When this occurs T cells that respond to the ocular antigen undergo clonal expansion and migrate to the site of inflammation.
Under normal circumstances, where ocular antigens remain in the eye, CD4+ helper T cells do not recognise ocular proteins because autoreactive T cells are deleted in the thymus during T cell development. However, there are rare instances when an autoreactive T cell develops because there is cross-reactivity between the ocular peptide and a previously encountered peptide, which may have occurred in response to previous immune responses to other infections. This cross-reactivity with a peptide seen previously in an infection is known as molecular mimicry. When this occurs T cells that respond to the ocular antigen undergo clonal expansion and migrate to the site of inflammation.
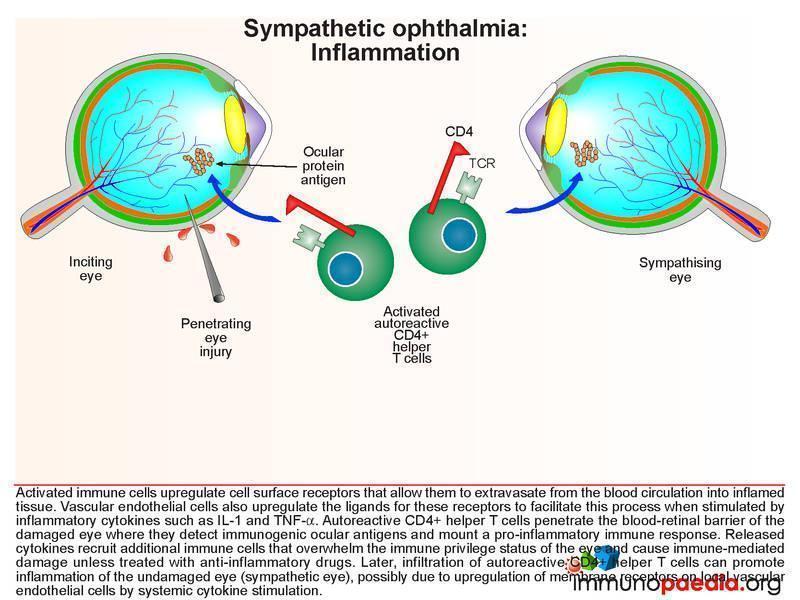 Activated T cells up-regulate surface receptors that allow them to extravasate from the blood circulation into inflamed tissue. Vascular endothelial cells also up-regulate receptors to facilitate this process when stimulated by inflammatory cytokines such as IL-1 and TNF-a. In this way ocular antigen-specific CD4+ helper T cells are able to penetrate the usually impervious blood-retinal barrier in the damaged eye and respond to the same ocular antigens. The inflammatory response continues to recruit more immune cells overwhelming the immune privilege status of the eye and causing further damage. This continues if unchecked, resulting in the swelling observed in our case, unless immunosuppressive drug therapy is initiated.
Activated T cells up-regulate surface receptors that allow them to extravasate from the blood circulation into inflamed tissue. Vascular endothelial cells also up-regulate receptors to facilitate this process when stimulated by inflammatory cytokines such as IL-1 and TNF-a. In this way ocular antigen-specific CD4+ helper T cells are able to penetrate the usually impervious blood-retinal barrier in the damaged eye and respond to the same ocular antigens. The inflammatory response continues to recruit more immune cells overwhelming the immune privilege status of the eye and causing further damage. This continues if unchecked, resulting in the swelling observed in our case, unless immunosuppressive drug therapy is initiated.
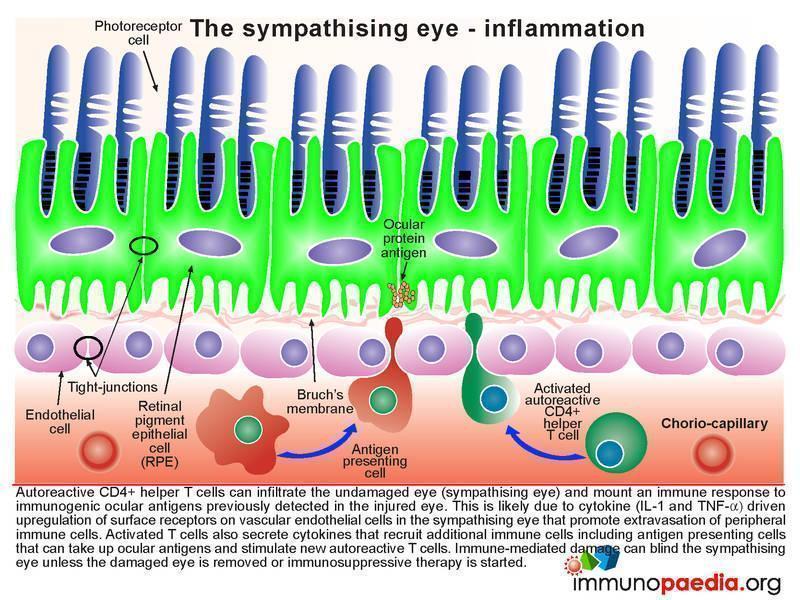
Inflammation in the sympathising eye
In our case study, the patient returned 3 weeks later with orbital swelling in the right “sympathising” eye. This is most likely due to systemic cytokine effects, with CD4+ helper T cells specific for the ocular antigen originally from the damaged left eye, which can now penetrate the blood-retinal barrier of the undamaged right eye (sympathizing eye). This initiates an immune response to the same antigen. Penetration of the right eye is likely due to upregulation of receptors on vascular endothelial cells in the sympathising eye by the action of IL-1 and TNF-a. The activated T cells secrete cytokines that recruit further T cells and antigen presenting cells that can continue to process ocular antigens. This cycle of events leads to inflammation and subsequent damage to the sympathising eye that can cause visual loss unless the damaged eye is removed early enough or immunosuppressive drugs are initiated in time.
Lets look at the pathophysiology of sympathetic ophthalmia in closer detail, as this is an example of how immune tolerance is broken which causes disruption to an immune privileged organ.
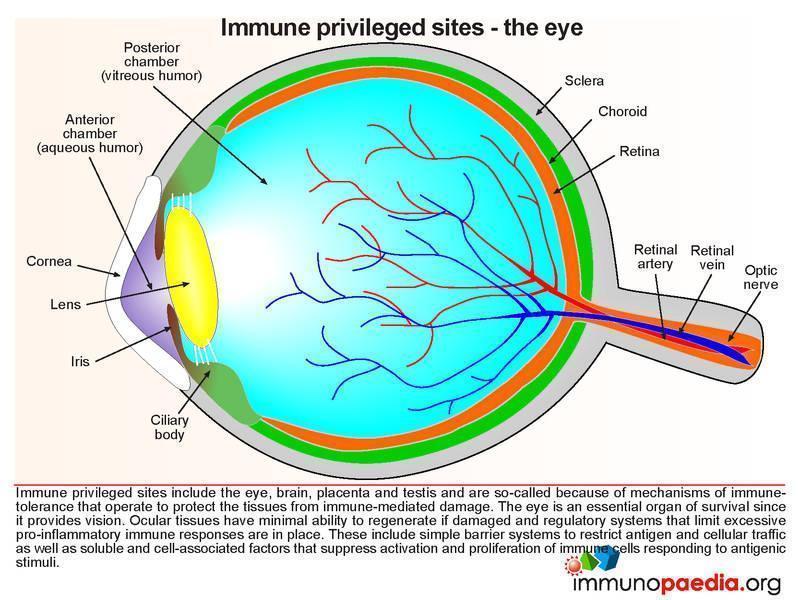
The eye is an essential organ of survival because it provides vision. For this reason it is one of the body’s immune privileged sites and mechanisms of immune tolerance operate to protect ocular tissues from immune-mediated damage. Other areas of the body which display similar immune tolerance include the brain, placenta and testis.
Ocular tissues have minimal ability to regenerate if damaged and therefore regulatory systems are in place to limit excessive pro-inflammatory immune responses. These include simple barrier systems to restrict antigen and cellular traffic as well as soluble and cell-bound factors that suppress immune cell activation. Six such mechanisms are discussed here in more detail: a) blood-retinal barrier; b) immune evasion; c) apoptosis; d) inhibitory factors; e) soluble immunosuppressive factors and f) immune deviation.
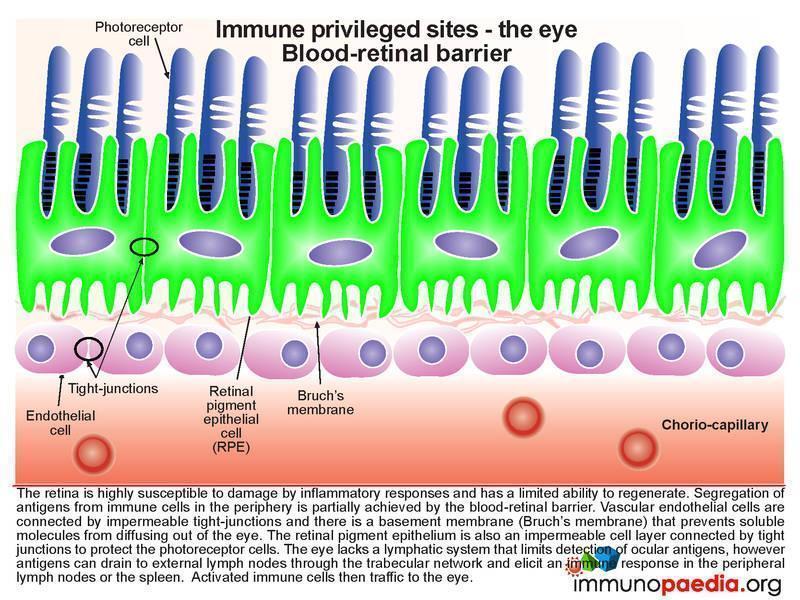
The Blood-retinal Barrier
As discussed in our case study, the retina has been damaged by inflammatory responses and has not been able to regenerate. Segregation of antigens from immune cells in the periphery is partially achieved by the blood-retinal barrier. Vascular endothelial cells are connected by impermeable tight-junctions and there is a basement membrane (Bruch’s membrane) that prevents soluble molecules from diffusing out of the eye. The retinal pigment epithelium is also an impermeable cell layer connected by tight junctions to protect the photoreceptor cells. The eye also lacks a lymphatic system, which serves as a drainage for inflammatory agents, and so the effects of inflammation are highly constrained. However, the important point to note, is that ocular antigens can prime new T cell responses at lymph nodes distal to the eye. In our case, the patient developed a cervical lymphadenopathy at the time of the sympathizing eye becoming inflamed.
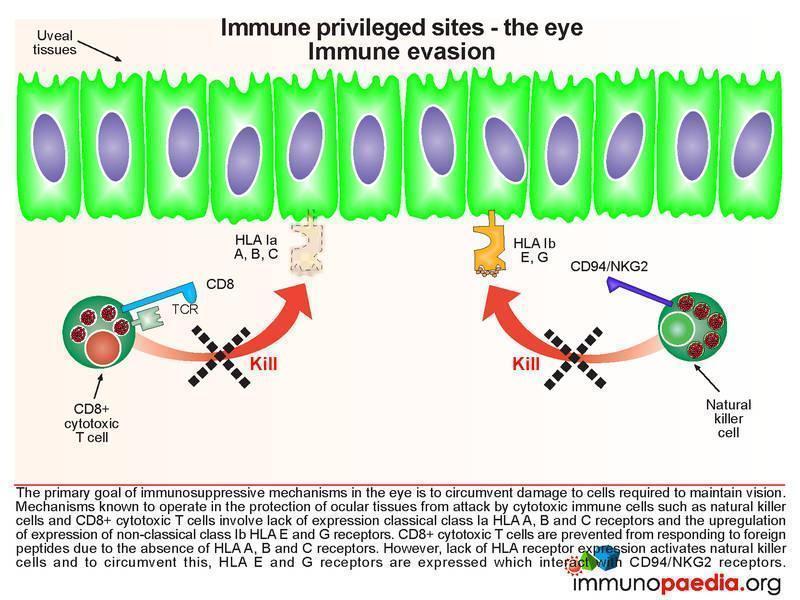
Immune Evasion
The primary goal of immunosuppressive mechanisms in the eye is to circumvent damage to cells required to maintain vision. Mechanisms known to operate in the protection of ocular tissues from attack by cytotoxic immune cells such as natural killer cells and CD8+ cytotoxic T cells involve lack of expression of the classical class I HLA A, B and C molecules and the expression of non-classical class I HLA E and G receptors. Specifically it has been shown that the absence of HLA A, B and C receptors prevents CD8+ cytotoxic T cells from responding to foreign peptides while the expression of HLA E and G receptors interacts with CD94/NKG2 receptors inhibiting the action of natural killer cells.
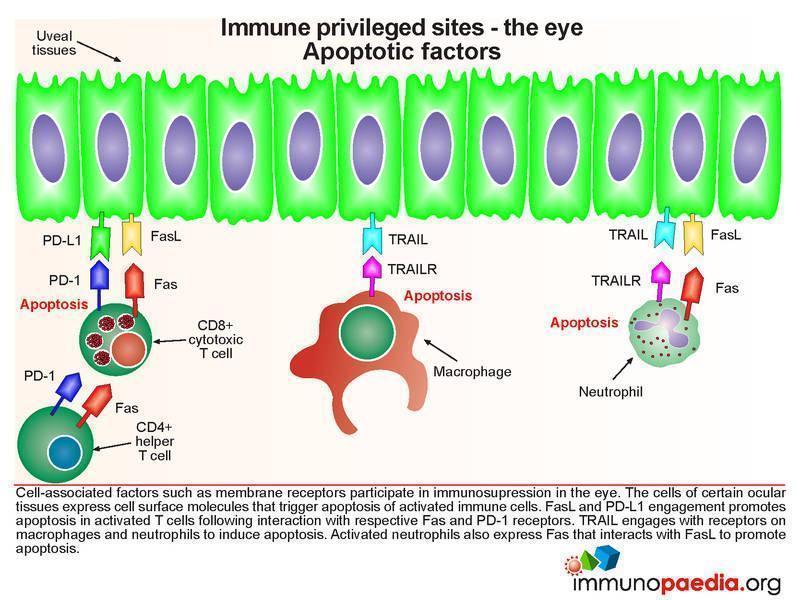
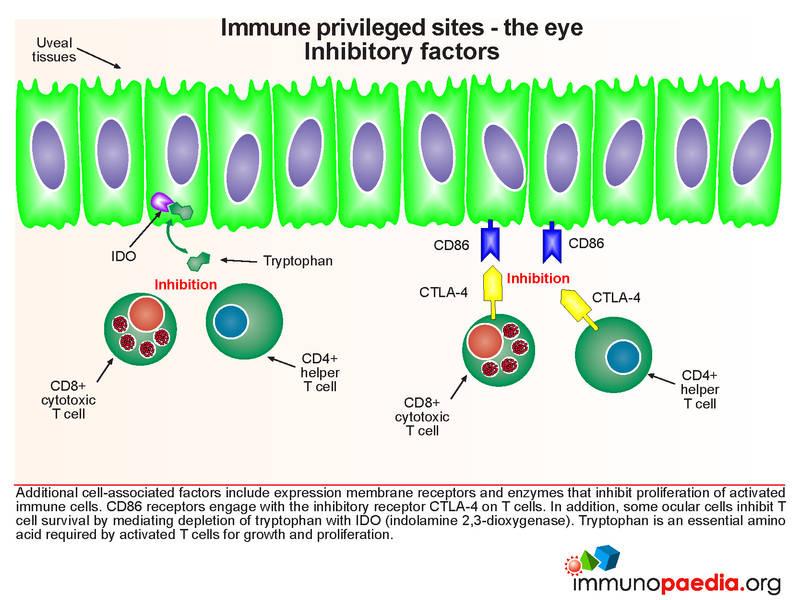
Apoptotic Factors and Inhibitory Factors
The cells of certain ocular tissues express membrane receptors that induce apoptosis or inhibition of activated immune cells as well as cellular enzymes that deplete tryptophan, an amino acid essential for T cell survival. Several of these mechanisms are now well understood. For simplicity, our graphic has been divided into two: one part which describes the factors involved in apoptosis and the second part which describes the inhibitory factors. Although depicted separately these are processes which occur simultaneously. FasL and PD-L1 engagement promotes apoptosis in activated T cells following interaction with respective Fas and PD-1 receptors. While another ligand, TRAIL (TNF-related apoptosis ligand), engages with receptors on macrophages and neutrophils to induce apoptosis. Activated neutrophils also express Fas that interacts with FasL to promote apoptosis. CD86 receptors engage with the inhibitory receptor CTLA-4 on T cells. In addition, some ocular cells inhibit T cell proliferation by mediating depletion of tryptophan with IDO (indolamine 2,3-dioxygenase).
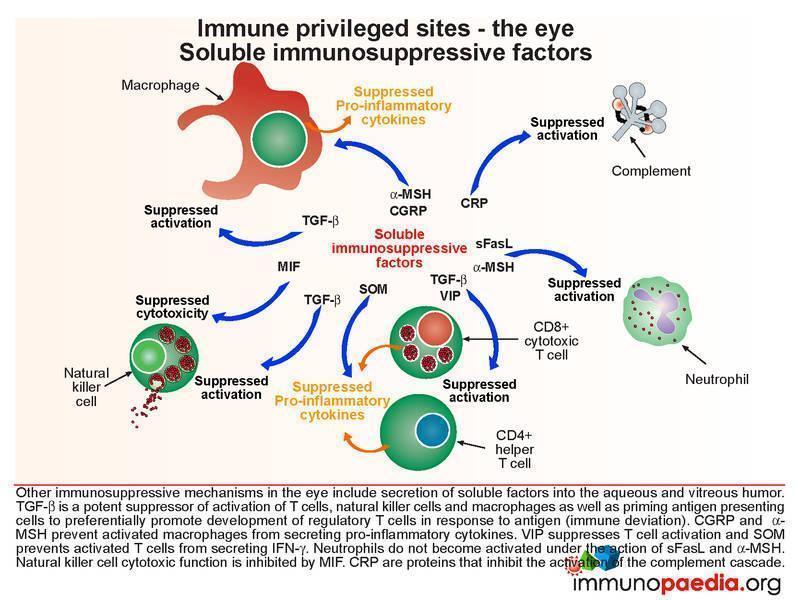
Soluble Immunosuppressive Factors
Other immunosupressive mechanisms in the eye include secretion of soluble factors into the aqueous and vitreous humor. Some of these factors are seen in the other immune privilege sites.
- TGF-beta is a potent suppressor of activation of T cells, natural killer cells and macrophages. It also primes antigen presenting cells to preferentially generate regulatory T cells in response to antigen presentation.
- CGRP and a-MSH prevent activated macrophages from secreting pro-inflammatory cytokines.
- VIP suppresses T cell activation
- SOM prevents activated T cells from secreting IFN-gamma.
- Neutrophils do not become activated under the action of sFasL.
- MIF inhibits natural killer cell cytotoxic function.
- CRP prevents activation of the complement cascade.
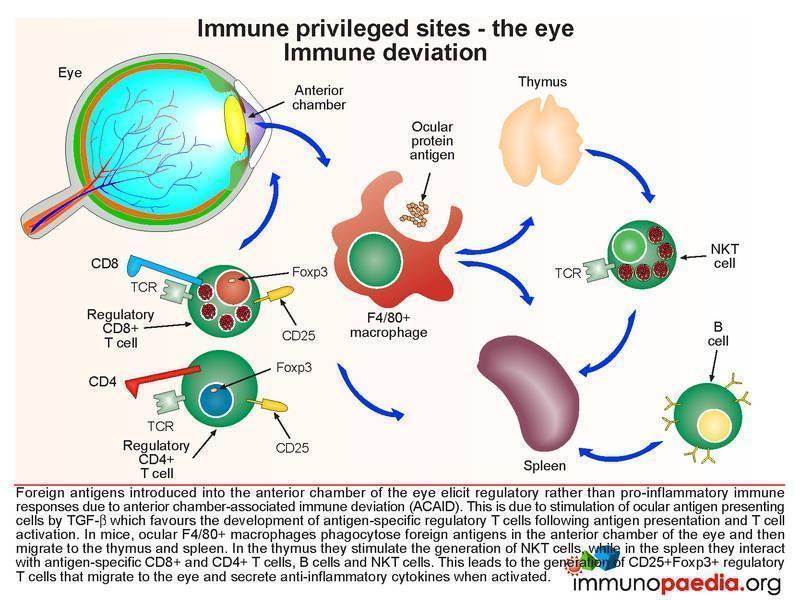
Immune Deviation
This process is a mechanism that protects the eye from collateral damage to an immune-mediated damaging response after infection. In a normal situation, when foreign antigens are deposited in the anterior chamber, due to infection, pro-inflammatory immune responses fail to be elicited due to anterior chamber-associated immune deviation (ACAID). Although this has only been described in experimental models, it is thought that ocular antigen presenting cells can preferentially select and activate regulatory T cells through the action of TGF-b. In mice it has been shown that ocular F4/80+ macrophages phagocytose foreign antigens in the anterior chamber of the eye and then migrate to the thymus and spleen. In the thymus they stimulate the generation of NK-T cells, while in the spleen antigen-specific CD8+ and CD4+ T cells are primed leading to the generation of regulatory T cells. These migrate back to the anterior chamber of the eye and suppress pro-inflammatory immune responses. It is unlikely that ACAID operates to this degree when the eye is physically disrupted.
Download images for this case
Treatment
Initial Treatment
When our patient first presented approximately 18 hours post injury, he was diagnosed with a penetrating knife injury to the left eye resulting in prolapse of the iris, ciliary body and retinal tissue. The eye was immediately surgically repaired, and an intraocular foreign body removal was performed. The patient was treated with antibiotics and steroid therapy.
- Topical steroids- 1% prednisolone acetate every 2 hours
- Periocular steroids – subconjunctival dexamethasone injections 3 times per week
- Systemic steroids
- Antibiotics
After discharge the patient was non-compliant and stopped therapy. Three weeks later the patient presented with bilateral panuveitis.
At this point the ophthalmologists enucleated the injured eye as it was blind and causing a sympathetic reaction in the uninjured eye.
The patient was then started on oral prednisone.
The most important aim in treating eye wounds is to maintain and improve visual outcome. This requires prompt initial treatment and aggressive doses of anti-inflammatory drugs to control the immune responses described in this discussion. High doses of oral prednisone are typically used which are then tapered according to therapeutic response. When necessary, especially if longer-term treatment is needed, other immunosuppressive medications, such as cyclosporine, infliximab and methotrexate can be used to control inflammation.
Download images for this case
Final Outcome
In this study, the patient and his parents were counseled regarding the importance of taking the medication correctly and attending regular-follow up visits to the clinic. The patient remained on his treatment until the steroid therapy was completed and his visual acuity in the right eye improved 20/40, a significant improvement on his admission visual acuity of 20/200
Download images for this case
References
Castiblanco CP et al. (2009). Sympathetic ophthalmia. Graefes Arch Clin Exp Ophthalmol. Mar;247(3):289-302.
Gupta SR et al. (2011). Successful treatment of refractory sympathetic ophthalmia in a child with infliximab. Arch Ophthalmol. Feb;129(2):250-2
Shankar V et al. (2010). Histopathological changes of cornea in long-term sympathetic ophthalmitis. Cornea. Nov;29(11):1287-90
Zhang Y et al. (2009). Development of sympathetic ophthalmia following globe injury. Chin Med J (Engl). Dec 20;122(24):2961-6.
Caspi RR. (2010). A look at autoimmunity and inflammation in the eye. J Clin Invest. Sep 1;120(9):3073-83.
Niederkorn JY et al. (2010). History and physiology of immune privilege. Ocul Immunol Inflamm. Jan;18(1):19-23.
Taylor AW. (2009). Ocular immune privilege. Eye (Lond). Oct;23(10):1885-9.
Niederkorn JY. (2009). Immune escape mechanisms of intraocular tumors. Prog Retin Eye Res. Sep;28(5):329-47.
Download images for this case
Evaluation – Questions & answers
What is the diagnosis?
What is/are the main predisposing factors for this condition?
What are the most common presenting signs and symptoms?
What is the pathophysiology of sympathetic ophthalmia?
Inflammatory cytokines such as IL-1 and TNF-a cause the blood retinal layer to become more permeable allowing CD4+ helper T cells to penetrate the usually impervious blood-retinal barrier in the damaged eye. The inflammatory response continues to recruit more immune cells overwhelming the mechanisms that maintain the immune privilege status of the eye and further damage continues. Due to the inflammatory status impacting on the unaffected eye, these ocular antigen-specific T cells enter the fellow eye causing retinal damage and the condition of sympathetic opthalmia.
What can be done to prevent this from occurring?
Download images for this case
Multiple Choice Questions
Earn 1 HPCSA or 0.25 SACNASP CPD Points – Online Quiz
Download images for this case



