





Through a randomized placebo-controlled trial, the authors investigated the effects of revaccination with BCG , a high-dose of BCG and a standard dose of BCG on the trained immunity in a cohort of 51 healthy adult volunteers (Fig 1). These individuals were all non-smokers and needed to have no history of BCG vaccination or a receipt of vaccination three months prior to being of the study. Parameters that were evaluated included; cytokine levels in response to different amounts of BCG and the effect that stimulation had on the production of pro-inflammatory cytokines in PBMCs and NK cells.
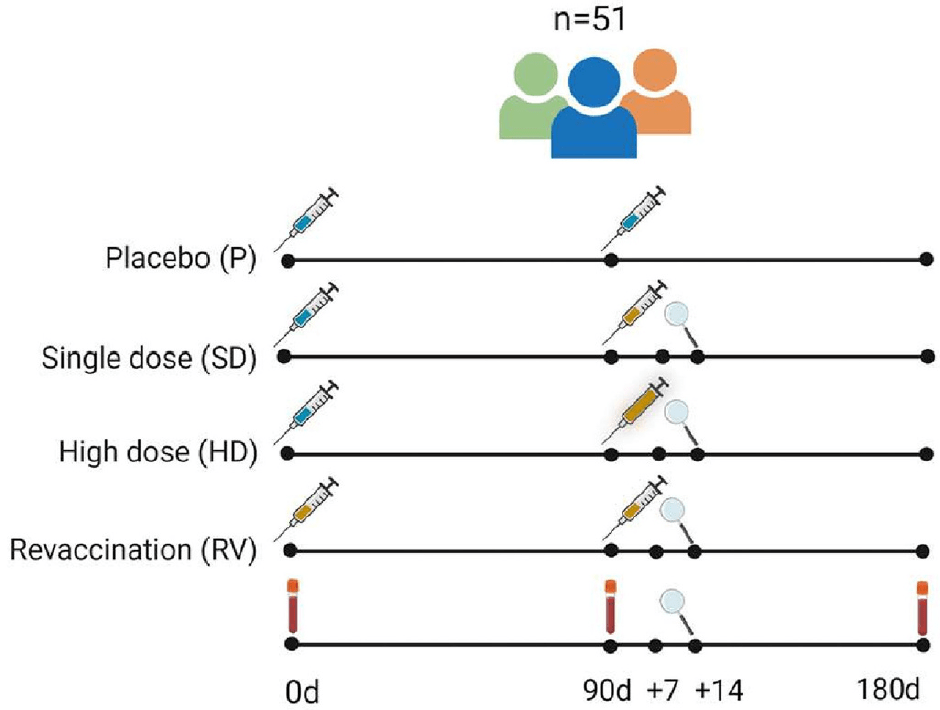
Figure 1: “Clinical study design comparing the effect of various BCG vaccination regimes on trained immunity: Fifty-one healthy adults were randomized to either one of the four intervention groups: placebo vaccination (P), single dose BCG (SD), high dose BCG (HD) or BCG revaccination (RV). Blood was drawn at baseline, 90d and 180d. Injection sites were inspected twice after the second vaccination, indicated by the magnifying glass.”
Following bacterial stimulation, there was an increase in pro-inflammatory cytokine production for participants across all three vaccination groups. Notably, TNFα was measured following stimulation with LPS, S. aureus and E. coli (Fig 2). Across all three vaccination groups however, no significant differences in with regards to pro-inflammatory cytokine production were noted (Fig 2). A look at NK cells after stimulation with C.albicans showed differences across groups such as lower in response to revaccination and significantly high levels of IFNβ and IFN from study participants that received a high dose of BCG. A look into T-cell responses within a pool of Mtb stimulated PBMCs demonstrated no differences in cytokine production across vaccination groups. Based on the differences seen between NK cells and T-cells, the authors suggests that in the presence of fungal infections, higher doses of BCG be helpful in driving NK cell responses in particular, but be accompanied with a possible downregulation of T-cell and monocyte responses.

Figure 2: “Monocyte-derived cytokine responses before vaccination and at 6 months. TNFα production was quantified in PBMCs after 24 h stimulation with LPS, S. aureus and E. coli. Black lines represent medians. Wilcoxon signed-rank test was performed to compare cytokine release before and after vaccination. Differences between the four intervention groups were analyzed with Kruskal-Wallis tests; n = 5 (P), n = 13 (SD), n = 16 (HD), n = 17 (RV); *p < 0.05, **p < 0.01.”
Overall the authors believe that from the results in this paper, vaccination with a standard dose of BCG does contain enough stimulus to elicit maximal cytokine production in monocytes, NK cells and T-cells following induction with stimuli. Revaccination was not taken to not prove to be superior to other forms of BCG vaccination carried out in this study. The authors also note that this and the overall magnitude of innate immune memory may be partly dependent on the presence and production of cytokines at baseline. Based on this, it was demonstrated that high dose BCG or revaccination with it may not significant enhance trained immunity .In conclusion, the authors had this to say; “Our results suggest that, in most cases, a single dose BCG is sufficient for achieving an effective trained immunity response. There are some arguments that if BCG is used to improve host defense against infections that are more contingent upon NK cell activity, it may be beneficial to increase the amount of BCG administered.
Journal article: Debisarun, P. A. et al., 2023. The impact of BCG dose and revaccination on trained immunity. Clinical immunology.
Summary by Vanessa Muwanga



