





 Non-specific effects of BCG vaccine have generated a lot of interest with researchers proposing that it likely protects against respiratory viruses like the SARS-CoV-2 virus. Though this is still under investigation, evidence on its heterologous protection, suggests a likely reduction of mortality in low birth weight infants.
Non-specific effects of BCG vaccine have generated a lot of interest with researchers proposing that it likely protects against respiratory viruses like the SARS-CoV-2 virus. Though this is still under investigation, evidence on its heterologous protection, suggests a likely reduction of mortality in low birth weight infants.
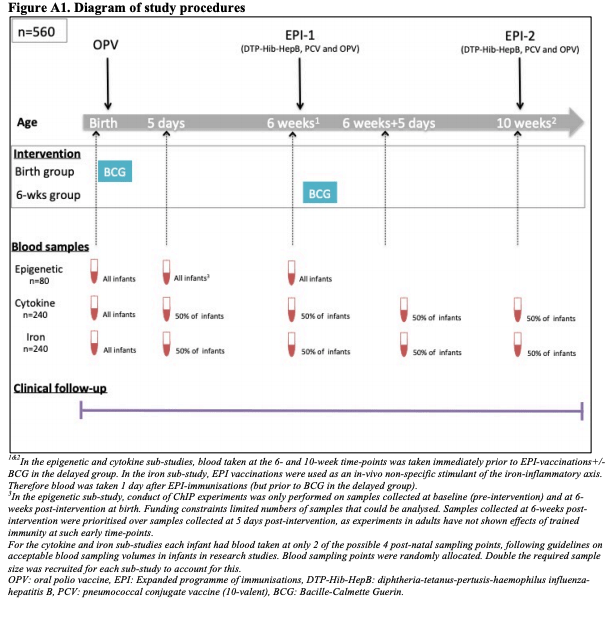
As this evidence is still contentious, studies like one done by Prentice et al (2021) are required to inform literature. This study was conducted in Entebbe, Uganda between September 2014 and July 2015. They investigated whether BCG alters all-cause infectious disease morbidity in healthy infants in settings, and explored whether the changes are mediated via trained innate immunity. It was an investigator-blind, randomised, controlled trial done at a hospital. 560 Participants recruited at birth were enrolled and randomly assigned to receive BCG at birth (n=280) or age 6 weeks (n=280).
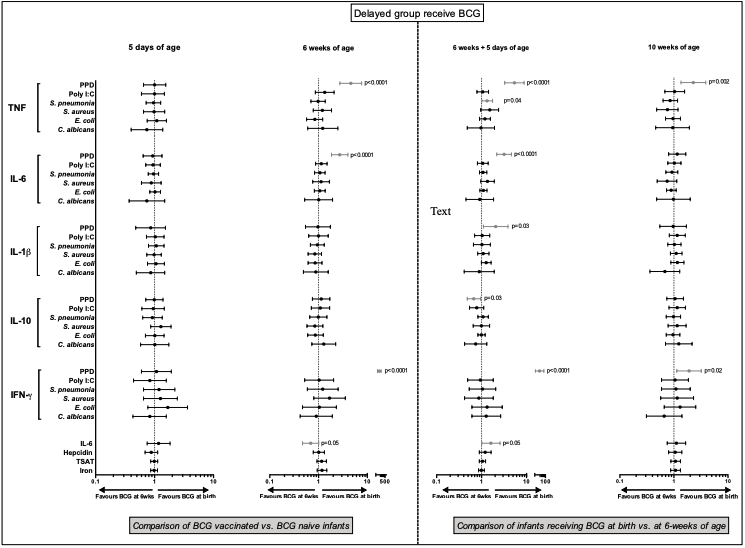
Geometric mean ratios (95% confidence intervals) of a) innate cytokine production measured by ELISA, following 24 hour stimulation of whole blood with bacterial/fungal whole killed pathogens, a viral-type stimulant (Poly I:C) and positive control (PPD) b) circulating inflammatory iron parameters, by BCG status. A geometric mean ratio >1 indicates that levels were higher in the BCG at birth group. The first two postnatal time points compared BCG-vaccinated vs naïve infants. The second two time points compared early (birth) with delayed (6-wks) BCG-vaccinated infants. Comparisons reaching statistical significance are shown in grey. The range of allowable blood-sampling timing at each age were 5d (d1-d7), 6 weeks (d42-49), 6 weeks + 5 days (d1-d7 post EPI-1+/-BCG vaccinations), 10 weeks (d70-77). Adjusting for day of blood sampling during analysis had little effect on the results. BCG: Bacille-Calmette Guerin, GMR: geometric mean ratio, TNF: tumor necrosis factor, IL-6: interleukin-6, IL-1β: interleukin-1beta, IL10:interleukin 10, IFNγ: interferon-gamma, PPD: purified peptide derivative, Poly I:C: polyinosinic:polycytidylic acid, S. pneumoniae: Streptococcus pneumoniae, S. aureus: Staphylococcus aureus, E.coli: Escherichia coli, C.albicans: Candida albicans, TSAT: transferrin saturation, wks:weeks
This study showed a significant reduction in physician-diagnosed all-cause infectious disease incidence in the first 6 weeks of life in infant. This did confirm that BCG vaccination protected against non-tuberculous infectious disease during the neonatal period, in addition to having tuberculosis-specific effects. Analysis of immune samples demonstrated lower histone trimethylation (repression) of promoter regions of genes encoding proinflammatory cytokine TNF and higher levels of M.tb antigen- TNF and IL-6 production. cytokines associated with trained immunity in 6-week-old unvaccinated infants compared to BCG vaccinated infants.
Although our study showed reductions in the global increase of histone trimethylation at some cytokine promoters in PBMCs over the first 6 weeks of life, associated with BCG vaccination, we cannot show that this was directly caused by BCG, rather than an indirect effect of the reduced frequency of other illness events.
Furthermore, this study being the first RCT in neonates to assess the potential for the BCG to train the innate immune system found out that BCG at birth indeed is associated with evidence of functional changes that resulted in some pro-inflammatory responses in peripheral blood mononuclear cells.
Journal Article: Prentice et al. 2021. BCG-induced non-specific effects on heterologous infectious disease in Ugandan neonates: an investigator-blind randomised controlled trial. The Lancet Infectious Diseases.
Summary by Ludoviko Zirimenya



