





The management of systemic autoimmune diseases (SAID) remains a challenge despite the availability of a number of tools for diagnosis and gauging the prognosis of the diseases. Antinuclear antibodies (ANA) are the first autoantibodies that were described in 1940. They still have the primary role in the diagnostic criteria of almost all SAID.
Indirect immunofluorescence assay (IIF) is the preferred or the gold standard method of detecting ANA. By using an appropriate substrate which is the human epithelial cell line (Hep-2), besides giving results as positive or negative, it also gives us a titer and pattern which, along with the clinical features of the patient help us to make a provisional diagnosis. For the final diagnosis, however, we need to run certain other tests including anti-ds DNA and ANA-specific antibodies.
The ANA-specific antibody (or anti-extractable nuclear antigens) is a misnomer as some of the autoantibodies are not targeted to the nuclear antigens but rather to other cellular components present in the cytoplasm, such as anti-Jo-1 and anti-ribosomal P protein antibodies. According to the international consensus on ANA patterns (ICAP), the reporting of reactivity on Hep-2 cells should be under the heading of anti-cellular antibodies (ACA). ICAP classifies the ACA into three categories, anti- nuclear, anti-cytoplasmic, and anti-mitotic. The ACA is given a code and the patterns can identify the specific autoantibodies. Such as speckled pattern which is the most reported pattern can give reactivity with anti-Sm, anti-SSA, -SSB, and several others. Anti-ds DNA antibodies are seen with homogenous and speckled patterns, and so on and so forth.
We did a laboratory and clinical audit and published it as “ANA‐specific antibodies, ANA patterns, anti‐ds‐DNA results, and clinical diagnosis: a laboratory and clinical audit” in Immunologic Research (Immunol Res, 2023 Apr;71(2):267-275. doi: 10.1007/s12026-022-09347-z. Epub 2022 Dec 2). In this study, we correlated a positive ANA-specific antibody result with the ANA patterns and we also analyzed anti-ds DNA antibody results for these patients’ samples. We also analyzed the clinical features and the diagnosis made by physicians for these patients. The audit was done to guide clinicians to utilize these autoantibodies for the diagnosis of SAID cost-effectively.
We analyzed the data of 641 patients for whom ANA-specific antibodies were requested. Of these 245 (38.2%) patients had reactivity for one or more of these antibodies. ANA results were available for 206 patients and 195 were ANA positive. Anti-ds DNA results were available for 190 patients who were both reactive for ANA and ANA-specific autoantibodies and 43% were positive (Figure 1).
The most common ANA pattern was speckled and the most prevalent ANA-specific autoantibody was anti-SSA. Some ANA patterns and ANA-specific antibodies had a significant correlation. But there was not a single association of an ANA-specific autoantibody with a particular pattern (Table 1). Moreover, more than one pattern was seen in 18 patients making the interpretation of results more challenging.
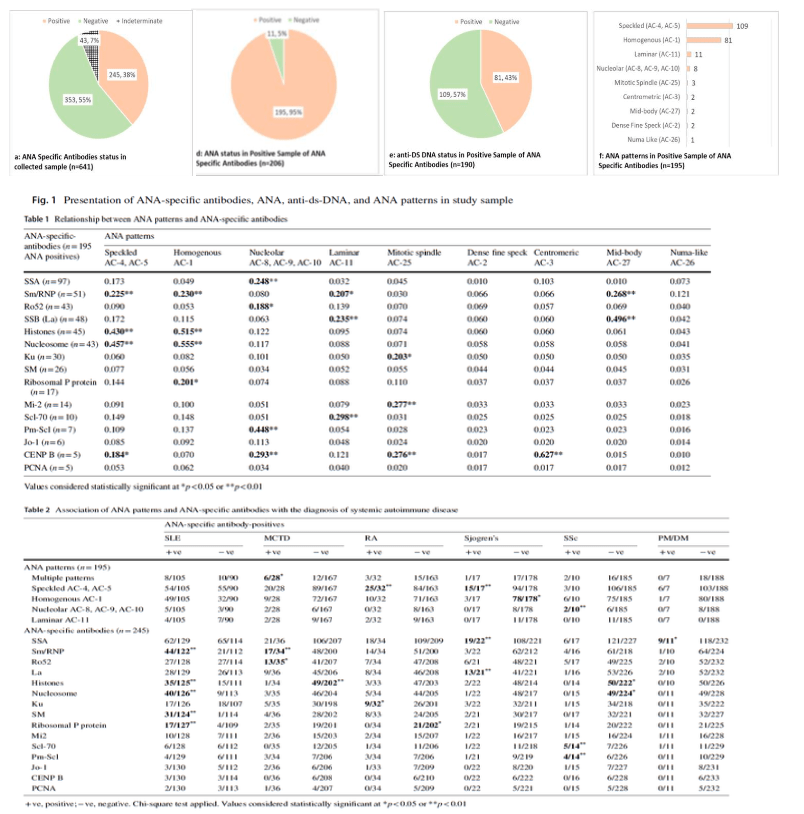
This study showed that testing for ANA-specific antibodies cannot be gated on ANA patterns. Also, there is a redundancy of these antibodies with various clinical diagnoses. Moreover, ANA-specific antibodies can also be found in ANA-negative patients. We observed that for test requests of ANA-specific autoantibodies, ANA and anti-ds DNA was not requested for all patients. following an algorithm with an initial ANA test followed by ANA-specific autoantibody and depending on ANA results, anti-ds DNA tests are a more logical and cost-effective strategy.
Future Research Prospectives for Autoantibodies in SAID
We are now focusing on Identifying specific markers as the predictor of various clinical manifestations in autoimmune diseases and correlating with the prognosis.
Journal article: Anis, S., et al. 2023. ANA-specific antibodies, ANA patterns, anti-ds-DNA results, and clinical diagnosis: a laboratory and clinical audit. Immuno. Resp.
Summary by Sabiha Anis



