





Chagas diseases, also known as American trypanosomiasis, is caused by the Trypansosoma cruzi parasite. Approximately 6-7 million individuals, predominantly from Latin America, are affected by the disease. If treated early with anti-parasitic treatment, progression to Chagas diseases following infection can be prevented. In the absence of treatment individuals remain chronically infected, with 20-30% of them developing cardiac complications such as cardiomyopathy (CDM).
Monocytes play an important role in the immune response to T.cruzi, where they migrate to the site of infection in responses to inflammatory signal. Recruited monocytes can contribute to effective control and clearance of parasite, however they can also contribute to tissue damage if left unchecked. Monocytes can be differentiated into 3 groups based on expression of CD14 and CD16. Classical monocytes, CD14hiCD16-, possess inflammatory functional capacity. Non-classical monocytes, CD14loCD16+, that play an important role in wound healing and have anti-inflammatory properties. Intermediate monocytes, CD14hiCD16+, share characteristics with both classical and non-classical monocytes. Argentinian researchers (Pérez-Mazliah et al.,) aimed to evaluate frequencies of these 3 monocyte populations during different phases of Chagas disease ranging from infection (T.cruzi seropositive) without CDM to individuals with severe CDM. Based on classical monocyte immunology, one would hypothesise an increased level of classical (inflammatory) monocytes and lower level of non-classical monocytes associated with Chagas induced CDM compared to T.cruzi infection.
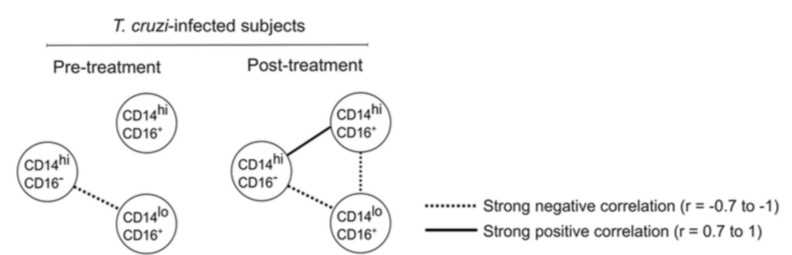
Classical, intermediate, and non-classical monocyte subsets prior to and after treatment with benznidazole are depicted by the corresponding circles. Each connecting line represents a significant interaction (P < 0.05) determined by Spearman’s correlation test. (Source Fig.3B)
Surprisingly they observed no difference in the overall frequency of classical, non-classical and intermediate monocytes during the different stages Chagas diseases. They did observe an inverse correlation between the frequency of classical and non-classical monocytes, a correlation which increased in individuals with CDM. Post treatment they observed a similar inverse correlation between classical and non-classical monocytes, as well as non-classical and intermediate monocytes. In addition to profiling the monocyte populations they also measured T.cruzi-specific antibodies before and after anti-parasitic therapy. They observed a decline T.cruzi-specific Ab in responses to treatment which was correlated with higher baseline levels of classical monocytes.
In summary, the study showed that individuals with severe cardiac disease suggestively have more pronounced levels of inflammation which result in increased classical monocytes. Highlighting that T.cruzi infection not only alters adaptive immunity but can alter components of innate immunity. A finding that contributes to improved understanding of disease progression.
Article: Pérez-Mazliah et al., 2018. Distinct monocyte subset phenotypes in patients with different clinical forms of chronic Chagas disease and seronegative dilated cardiomyopathy. Plos Neg. Diseases
Article by Cheleka AM Mpande



