





New research identifies the immune cells that travel from skin to joints and why they trigger disease in some patients (Figure 1).
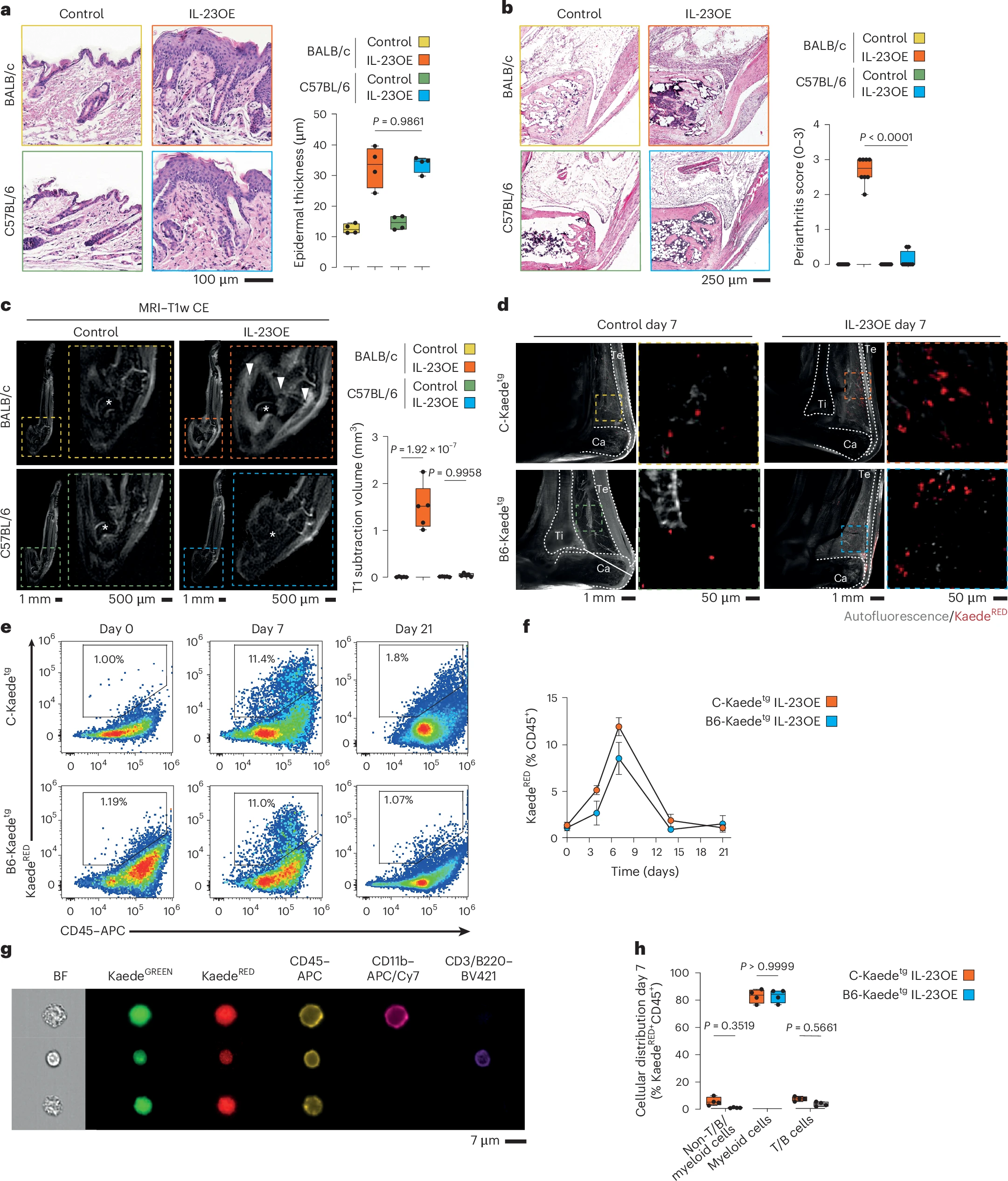
Figure 1: CD11b+ myeloid cells migrate from the skin to joints in a model of psoriatic disease. a, Left, representative micrographs of H&E-stained skin sections of the hind paws of BALB/c and C57BL/6 mice at day 21 with and without IL-23OE. Right, quantification of epidermal thickness at day 21. The graph shows the median, quartiles and minimum–maximum; N = 4 per condition. P values were calculated by one-way analysis of variance (ANOVA) with a Tukey’s post hoc test. b, Left, representative micrographs of H&E-stained ankle sections of BALB/c and C57BL/6 mice at day 21 with and without IL-23OE. Right, quantification of arthritis at day 21. The graph shows the median, quartiles and minimum–maximum; N = 8 per condition. P values were calculated by one-way ANOVA with a Tukey’s post hoc test. c, Representative micrographs of MRI-scanned ankles of BALB/c and C57BL/6 mice at day 21 with and without IL-23OE used for the quantification of arthritis at day 21. Arrowheads indicate inflammation, and stars indicate the talar bone. The graph shows the median, quartiles and minimum–maximum; N = 5 per condition. P values were calculated by one-way ANOVA with a Tukey’s post hoc test; T1w CE, T1-weighted contrast-enhanced. d, Representative micrographs of light sheet fluorescence microscopy of Kaedetg ankles from BALB/c (C-Kaedetg) and C57BL/6 (B6-Kaedetg) background strains at day 7 with and without IL-23OE and after photoconversion of cells localized in the skin. Arrowheads indicate accumulations of photoconverted KaedeRED cells. Graphical drawings of the tibia (Ti), calcaneus (Ca) and Achilles tendon (Te) are included. e, Representative flow cytometry plots for the quantification of KaedeRED skin-derived cells in the joint. f, Quantification of KaedeRED skin-derived cells in the joints. The graph shows the mean and standard error of the mean; N = 4 per time point and condition. g, Representative micrographs of imaging flow cytometry for the typing of KaedeRED skin-derived cells in the joint at day 7; BF, brightfield. h, Quantification of CD45+ KaedeRED skin-derived cell types in the joints at day 7. The graph shows medians, quartiles and minimum–maximum; N = 4 per condition. P values were calculated by one-way ANOVA with a Tukey’s post hoc test.
Up to one-third of people with psoriasis eventually develop psoriatic arthritis, a painful inflammatory condition that can permanently damage joints if left untreated. Until now, it has been unclear why joint disease develops in only a subset of patients.
Researchers have now uncovered the cellular mechanism that links skin inflammation to joint disease. Their findings reveal how specific immune cells migrate from inflamed skin to the joints and why they only cause arthritis in certain individuals.
In psoriasis, inflammation in the skin leads to the generation of specialized immune precursor cells. The researchers found that these cells can:
- Exit inflamed skin
- Enter the bloodstream
- Migrate onward to the joints
Importantly, this migration alone is not sufficient to cause joint inflammation. Many psoriasis patients harbour these circulating immune cells without ever developing arthritis.
The key determinant lies within the joint itself. Once immune cells arrive, they interact with fibroblasts, connective tissue cells that normally help maintain joint integrity and restrain inflammation.
In patients who go on to develop psoriatic arthritis, these fibroblasts lose much of their protective function. As a result:
- Incoming immune cells are no longer effectively controlled
- Inflammatory signals escalate
- Sustained joint inflammation is triggered
By contrast, in patients whose fibroblasts remain functionally intact, migrating immune cells fail to ignite joint disease.
This discovery provides a long-missing explanation for why psoriasis progresses to arthritis in some patients but not others. It is not simply the presence of inflammatory immune cells that matters, but how the joint tissue responds to them.
Crucially, the migratory immune cells identified in the study can be detected in the bloodstream before joint symptoms appear. This raises the possibility of:
- Identifying patients at high risk of psoriatic arthritis early
- Monitoring disease progression before irreversible joint damage occurs
- Developing preventive therapies that intercept these immune cells or restore fibroblast function
Rather than treating psoriatic arthritis only after joint damage has begun, the findings open the door to interceptive therapies approaches aimed at stopping the disease before it takes hold.
By targeting the migration of inflammatory immune cells or strengthening the joint’s natural protective barriers, future treatments may be able to prevent psoriasis from progressing into a debilitating joint disease.
Journal article: Raimondo, M.G., et al. 2026. Skin-derived myeloid precursors and joint-resident fibroblasts spread psoriatic disease from skin to joints. Nature Immunology.
Summary by Stefan Botha



