





A new approach using genetically engineered immune cells could offer a future bladder-preserving treatment option for patients with high-risk bladder cancer (Figure 1). Researchers from have developed specialised CAR T cells that can recognise and destroy bladder cancer cells while limiting damage to healthy tissues.
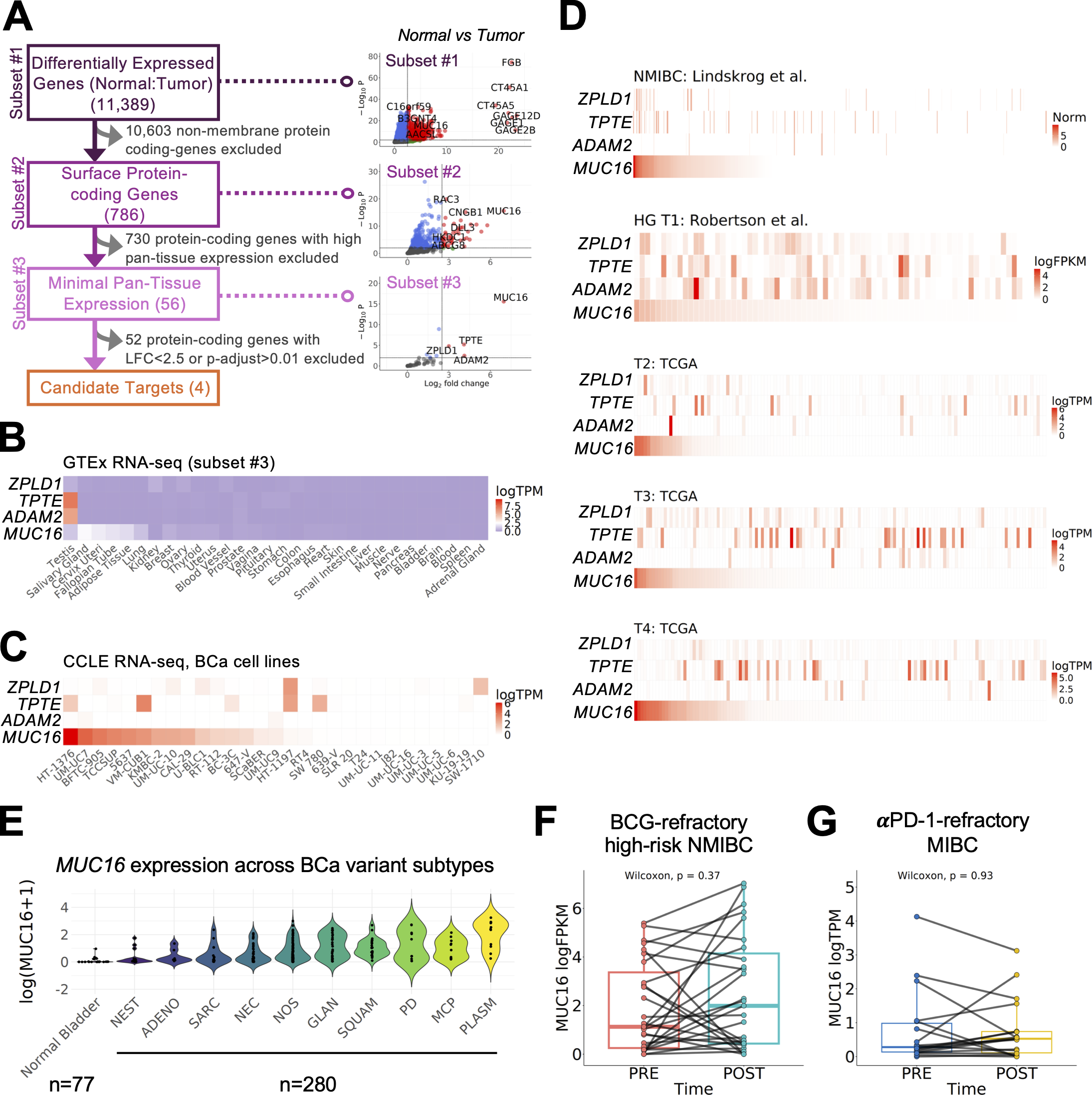
Figure 1: Comprehensive transcriptomics-based analysis identifies MUC16 as a potential target for CAR T cell therapy of BCa. (A) Schematic of the antigen discovery pipeline utilizing paired tumor:normal bladder datasets, identifying differentially upregulated gene transcripts and annotated membrane-bound proteins that have minimal expression in normal bladder or other tissues. (B and C) (B) Pan-normal tissue expression across the GTEx dataset and (C) expression across established BCa cell lines from the CCLE for top candidate genes MUC16, ADAM2, TPTE, and ZPLD1. (D) Expression of the same candidate genes across multiple BCa cohorts representing NMIBC (n = 535, Lindskrog et al., 2021), HGT1 (n = 73, Robertson et al., 2020), and MIBC (n = 404, subsets T2: n = 130, T3: n = 140, T4: n = 134, [Weinstein et al., 2013]). (E)MUC16 expression is enriched across subsets of tumors representing divergent differentiation and variant histological subtypes (normal bladder [n = 77, GTEx], variant legend: n = 280 tumors, NEST: nested variant [n = 16], ADENO: adenocarcinoma [n = 7], SARC: sarcomatoid [n = 30], NEC: neuroendocrine [n = 41], NOS: not otherwise specified [n = 95], GLAN: glandular [n = 30], SQUAM: squamous [n = 25], PD: poorly differentiated [n = 10], MCP: micropapillary [n = 10], and PLASM: plasmacytoid [n = 11]). (F and G) (F) MUC16 persists in high-risk NMIBC tumors that recur after BCG intravesical therapy (n = 44, de Jong et al., 2023), and (G) in MIBC tumors not responsive to neoadjuvant pembrolizumab (n = 18, Necchi et al., 2018).
The study demonstrates that delivering these engineered immune cells directly into the bladder using a catheter successfully controlled tumour growth in mouse models, highlighting a potential new strategy for treating solid tumours that have historically been difficult targets for cellular immunotherapy.
Bladder cancer is among the most common cancers worldwide, with approximately 600,000 new cases diagnosed each year. Current treatment typically involves surgical tumour removal followed by chemotherapy or immunotherapy. However, many patients experience tumour recurrence or disease progression, and some eventually require complete removal of the bladder, a procedure associated with major impacts on quality of life.
This clinical challenge has driven interest in developing bladder-sparing therapies that can eliminate cancer while preserving organ function.
CAR T cell therapy has already transformed treatment for several blood cancers, including leukaemias and lymphomas. The approach involves genetically modifying a patient’s own T cells to express a chimeric antigen receptor (CAR), an artificial receptor that enables immune cells to specifically identify and kill cancer cells.
However, applying CAR T cell therapy to solid tumours, such as bladder cancer, has proven much more challenging. Solid tumours often create barriers that prevent immune cell infiltration, and many potential tumour targets are also present on healthy tissues, increasing the risk of dangerous off-target effects.
The research team addressed these challenges by combining two strategies: designing highly specific CAR T cells and delivering them directly into the bladder environment.
The engineered CAR T cells were designed to recognise MUC16, a protein abundantly expressed on the surface of many bladder cancer cells, including tumour types that are resistant to existing treatments. Importantly, MUC16 expression is limited in most normal tissues, making it an attractive target for cancer-directed immune therapy.
In laboratory experiments, the engineered T cells efficiently killed MUC16-positive bladder cancer cells derived from patient tumours.
The researchers then tested the therapy in mice implanted with human bladder cancer cells. When CAR T cells were administered through the bloodstream, they showed limited effectiveness, reflecting one of the major challenges of treating solid tumours with cellular therapies. However, when the CAR T cells were delivered directly into the bladder through intravesical administration, they significantly reduced tumour growth and improved survival.
This direct delivery method provided two key advantages. First, it increased the concentration of therapeutic immune cells at the tumour site. Second, the CAR T cells remained largely confined within the bladder, reducing the likelihood of systemic toxicity and unintended immune attacks against other organs.
The findings establish MUC16 as a promising target for bladder cancer CAR T cell therapy and demonstrate that direct delivery through existing urological procedures may provide a practical route for bringing cellular therapies to solid tumours.
While the research remains at the preclinical stage, the study represents an important step toward expanding CAR T cell therapy beyond blood cancers. By combining precise tumour targeting with localised delivery, researchers may overcome some of the major barriers that have limited the success of cellular immunotherapies in solid tumours.
Journal article: Abrahimi, P, et al. 2026. Intravesical mesothelin-based CAR T cells targeting MUC16 effectively control bladder cancer in preclinical models. JEM.
Summary by Stefan Botha



