





May is Women’s Health Month, and 22 May marks World Preeclampsia Day. This annual moment is dedicated to raising awareness of a condition that has shaped maternal and neonatal medicine for centuries and still ranks among the leading causes of pregnancy-related death worldwide. The day exists in part because our understanding of preeclampsia has been stubbornly resistant to progress: for most of modern obstetric history, delivery has been the only definitive treatment, and risk prediction has relied on broad clinical heuristics rather than biology. That is now beginning to change. Across both therapeutics and screening, a new generation of research is reframing preeclampsia as a disease we can meaningfully slow, and increasingly, anticipate…months before it declares itself.
Preeclampsia remains one of the most dangerous complications of pregnancy and a leading cause of maternal and neonatal morbidity and mortality worldwide. In severe cases occurring before term, clinicians often face an impossible trade-off: deliver the baby early to protect the mother or continue the pregnancy and risk worsening maternal disease.
The weight of this dilemma falls disproportionately on low- and middle-income countries (LMICs), where access to neonatal intensive care is limited and even a few additional days in utero can mean the difference in outcome. In sub-Saharan Africa, hypertensive disorders of pregnancy remain a major contributor to maternal mortality, and the complications of extreme prematurity drive a substantial share of neonatal deaths. Patient advocacy organisations such as the Preeclampsia Foundation have long highlighted both the global scale of this burden and the urgent need for better tools. Research groups have also established international collaborations focuses on tackling this disease such as Preeclampsia Research. Against this backdrop, several studies emerging from Stellenbosch University and global collaborators all the way to the USA are helping reshape the treatment paradigm.
Here we explore therapies designed not simply to manage symptoms, but to biologically slow disease progression and safely prolong gestation. Additionally, we look into novel innovations in disease predictions.
Metformin: proof-of-concept for treating preterm preeclampsia
In a landmark randomised placebo-controlled trial published in The BMJ, researchers evaluated whether extended-release metformin could prolong pregnancy in women with preterm preeclampsia undergoing expectant management [1]. The trial enrolled 180 women between 26 and 32 weeks’ gestation at Tygerberg Hospital in Cape Town, with participants receiving either 3 g/day of extended-release metformin or placebo until delivery.
Although the primary analysis narrowly missed conventional statistical significance, the results suggested a clinically meaningful prolongation of pregnancy (Figure 1). Women receiving metformin remained pregnant for a median of 17.7 days after randomization compared with 10.1 days in the placebo group, an extension of approximately one additional week. Among women who tolerated and continued therapy, gestation was prolonged even further, with some analyses showing gains of 9–11 days.
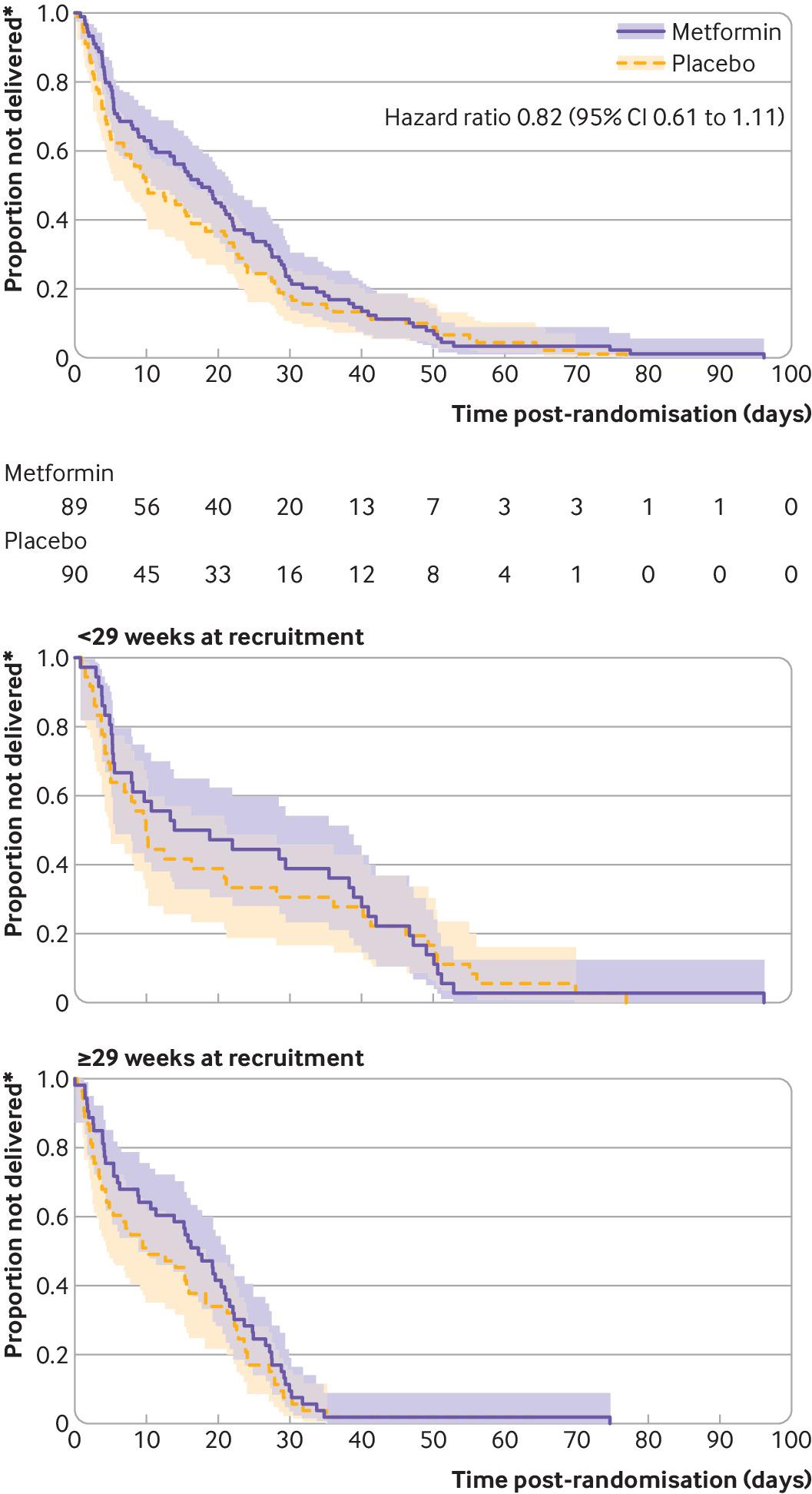
Figure 1: Outcomes in women with preterm pre-eclampsia assigned to extended-release metformin or placebo. Values are numbers (percentages) unless stated otherwise (1).
In neonatal medicine, even a few extra days in utero can substantially improve survival and reduce complications associated with extreme prematurity. That effect is amplified in resource-limited settings, where every additional day reduces dependence on advanced neonatal care that may simply not be available.
Importantly, metformin was not associated with major safety concerns. Gastrointestinal side effects such as diarrhea were more common, but no serious adverse events attributable to the drug were observed. While maternal angiogenic markers including soluble Flt-1 and placental growth factor were unchanged, infants in the metformin arm showed trends toward higher birth weights and shorter neonatal nursery stays. Together, these findings provided some of the first clinical evidence suggesting that preterm preeclampsia may, in fact, be pharmacologically modifiable rather than inevitably progressive. A follow up study in a larger cohort has been extended to more sites and is still ongoing.
Why metformin may work
Originally developed as a glucose-lowering therapy for type 2 diabetes, metformin has increasingly attracted attention for its pleiotropic vascular and immunometabolic effects. Preclinical studies suggest it may reduce oxidative stress, improve endothelial function, suppress anti-angiogenic signaling, and modulate placental inflammation, all central features of preeclampsia pathophysiology. The drug also influences mitochondrial metabolism and AMP kinase signaling, pathways increasingly implicated in placental dysfunction.
Rather than directly reversing disease, metformin may therefore improve maternal vascular resilience sufficiently to slow deterioration and buy valuable time for fetal maturation.
DM199: targeting vascular dysfunction more directly
Building on the concept that preeclampsia may be therapeutically treatable, a second emerging strategy targets the maternal vasculature more directly. Researchers recently launched an early-phase clinical trial investigating DM199, a recombinant form of tissue kallikrein-1 designed to restore endothelial function and improve placental perfusion [2]. The compound is being developed by DiaMedica Therapeutics, which has positioned preeclampsia and fetal growth restriction as a central focus of its clinical pipeline.
Unlike metformin, which acts through broader metabolic pathways, DM199 specifically activates the kallikrein–kinin system by releasing bradykinin, which then stimulates bradykinin B2 receptors on endothelial cells. This promotes vasodilation alongside anti-inflammatory, antioxidant, and pro-angiogenic effects. The rationale is compelling because endothelial dysfunction and impaired placental blood flow are central drivers of both preeclampsia and fetal growth restriction.
The ongoing phase Ib/IIa trial at Tygerberg Hospital includes women with severe preeclampsia, preterm preeclampsia managed expectantly, and fetal growth restriction. Investigators are assessing safety, pharmacokinetics, placental transfer, blood pressure effects, and preliminary efficacy signals. As a recombinant protein, DM199 is considered unlikely to cross the placenta significantly, potentially reducing fetal exposure compared with small-molecule therapies.
A shift from reactive to disease-modifying treatment
Together, these studies reflect a broader conceptual shift in obstetric medicine. Historically, preeclampsia has been viewed as a condition that could only be monitored until delivery became unavoidable. Advances in placental biology, vascular immunology, and endothelial signaling are now opening the possibility of disease-modifying therapies.
Metformin and DM199 approach the disease from different angles. Metformin appears to act through systemic metabolic and endothelial stabilization, whereas DM199 aims to directly restore vascular homeostasis and placental perfusion. Yet both strategies share a common goal: safely prolonging pregnancy long enough to improve neonatal outcomes without compromising maternal safety.
The work is especially significant in LMICs such as South Africa. Larger trials will be required before either therapy becomes standard of care, but the collective evidence suggests preterm preeclampsia may no longer be an untreatable obstetric emergency.
Rethinking who is actually at risk
Therapeutic innovation is only half the picture. Equally pressing is the question of who should be treated — and current screening tools are showing their age. Recent advances in hypertensive disorders of pregnancy (HDP) are beginning to challenge the long-standing “one-size-fits-all” approach to risk prediction and prevention, highlighting a growing disconnect between clinical risk assessment strategies and the underlying biological heterogeneity of disease.
A large prospective cohort study published in JAMA Network Open evaluated the clinical utility of the US Preventive Services Task Force (USPSTF) guidelines for preeclampsia risk stratification and aspirin prophylaxis [3]. In a cohort of more than 5,600 pregnancies, nearly 89% of participants were classified as being at “increased risk” for preeclampsia, with 70% categorized as moderate risk and 18.5% as high risk (Figure 2). Despite this, the predictive value of most moderate-risk factors was surprisingly weak. Nulliparity remained one of the few consistently informative predictors, whereas advanced maternal age was paradoxically associated with lower risk, and Black race alone showed no independent association with preeclampsia development after adjustment.
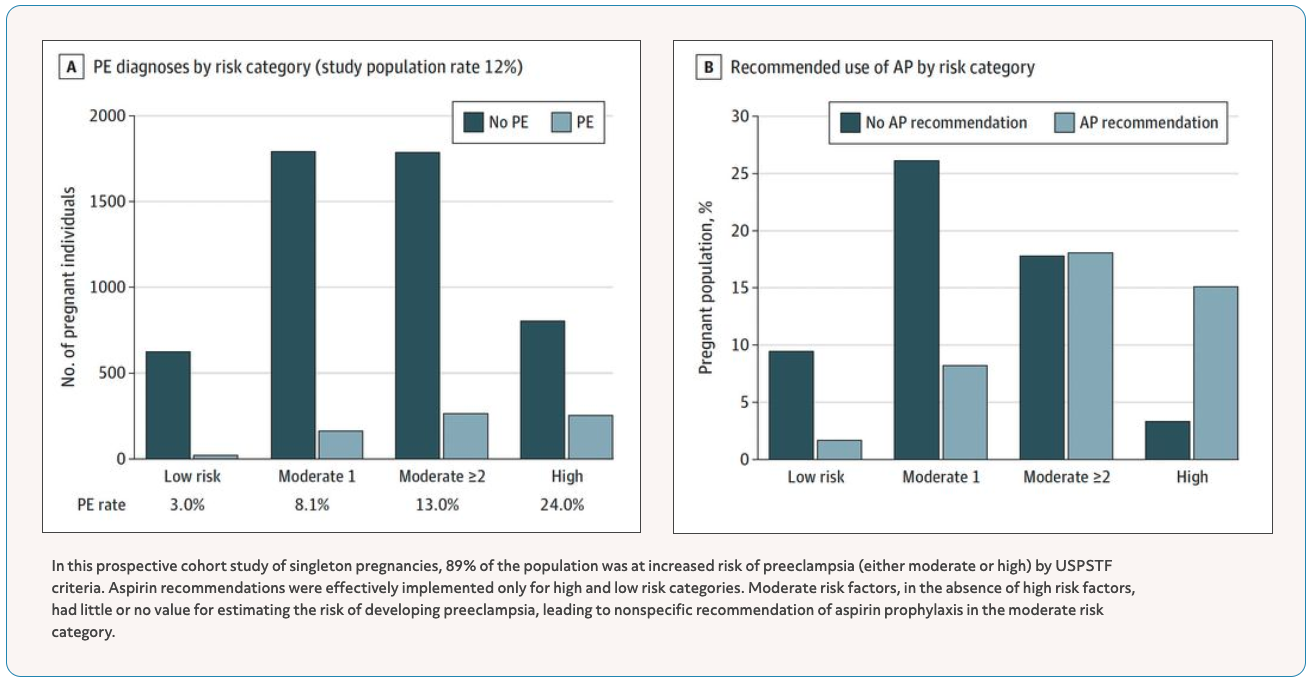
Figure 2: Source – (3) and mirvie.com.
The study revealed a major limitation of current guidelines: the moderate-risk category is so broad and nonspecific that it captures the majority of pregnant individuals while offering little discriminatory power. This translated directly into inconsistent aspirin prophylaxis recommendations in clinical practice. While clinicians appropriately recommended aspirin to most individuals with clear high-risk conditions, recommendations were far more variable among those with moderate-risk profiles, even though this group represented the bulk of the population. Together, these findings suggest that current clinical algorithms may overclassify risk without meaningfully identifying who is biologically most likely to develop severe disease.
Molecular subtypes: not one disease, but several
A complementary study published in Nature Communications approached the same problem from a molecular perspective [4]. This study used transcriptomic profiling from more than 9,000 prospectively collected pregnancies, work led by researchers at Mirvie, a company developing prenatal RNA-based diagnostics (Figure 3). The study demonstrated that hypertensive disorders of pregnancy are not a single disease entity but instead comprise distinct molecular subtypes with fundamentally different biological drivers.
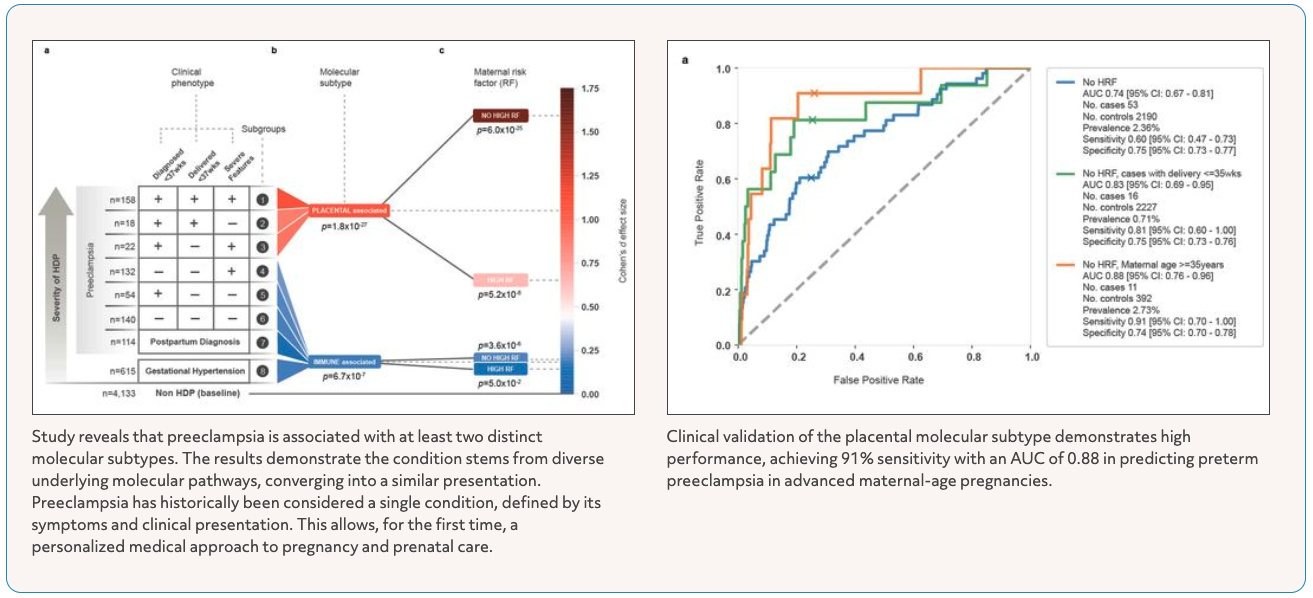
Figure 3: Source – (4) and mirvie.com.
Two dominant molecular programs emerged: a placental-associated subtype and an immune-associated subtype. Placental-associated disease was strongly linked to elevated expression of PAPPA2, a placental gene that predicted severe preeclampsia months before symptom onset, particularly in individuals who lacked traditional high-risk clinical features. PAPPA2 levels correlated with disease severity and earlier delivery in a dose-dependent manner. In contrast, less severe HDP phenotypes were characterized by immune and inflammatory transcriptional signatures, suggesting that immune dysregulation may define a biologically distinct subtype of disease.
Notably, the predictive performance of these molecular signatures substantially outperformed conventional clinical risk factors. In individuals with advanced maternal age but no established high-risk conditions, the placental-associated transcriptomic signature achieved an AUC of 0.88 for predicting severe disease, far exceeding the specificity achievable with current guideline-based approaches.
Biomarkers already changing practice: the sFlt-1:PlGF ratio
While transcriptomic profiling remains largely a research tool, biomarker-driven approaches are already reshaping real-world clinical management. One of the most clinically impactful advances has been the development of the soluble fms-like tyrosine kinase-1 to placental growth factor (sFlt-1:PlGF) ratio. In the landmark PROGNOSIS study, published in the New England Journal of Medicine in 2016, an sFlt-1:PlGF ratio of 38 or lower had an exceptional negative predictive value of 99.3% for ruling out preeclampsia within one week in women with suspected disease [5] (Figure 4). Although the test was less effective at positively predicting who would ultimately develop preeclampsia, its ability to safely exclude imminent disease progression represents a major advance for obstetric triage.
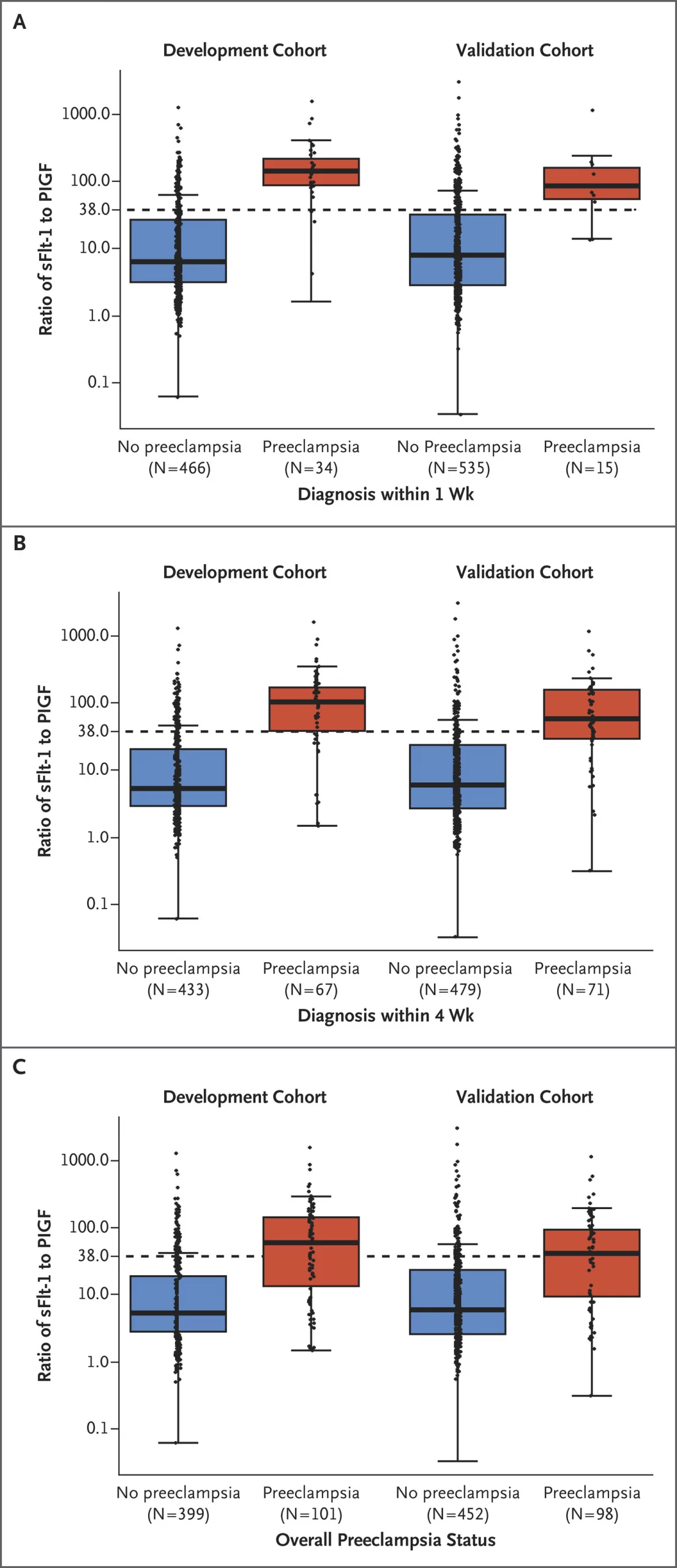
Figure 4: Ratio of sFlt-1 to PlGF for Participants with and Those without Preeclampsia in the Development and Validation Cohorts (5).
Biologically, the ratio reflects one of the central pathogenic pathways in preeclampsia: angiogenic imbalance. Placental dysfunction leads to excess release of sFlt-1, an anti-angiogenic factor that antagonizes VEGF and PlGF signaling, driving endothelial dysfunction, vasoconstriction, and placental insufficiency. The clinical utility of the ratio lies in translating this molecular pathology into a practical decision-making tool that may reduce unnecessary hospitalization while improving surveillance for truly high-risk patients. Since then, there have been several studies and trials validating this ratio and it’s clinical utility.
Toward precision obstetrics
Taken together, these studies illustrate a major conceptual shift in preeclampsia research. Traditional demographic-based risk models are increasingly being recognized as blunt instruments with limited specificity, particularly for the large population categorized as “moderate risk.” Molecular biomarkers and transcriptomic profiling are beginning to reveal biologically distinct subtypes of disease that may better explain the enormous heterogeneity seen in clinical practice.
This has direct implications for aspirin prophylaxis. Low-dose aspirin is currently recommended on the basis of population-level risk algorithms, yet the emerging data suggest future strategies may instead target biologically defined subgroups most likely to benefit. Rather than categorizing patients simply by age, BMI, parity, or race, transcriptomic approaches may eventually allow clinicians to identify the specific molecular trajectory of disease months before clinical manifestations appear.
Hypertensive disorders of pregnancy continue to rise globally, with the heaviest burden falling on LMICs where diagnostic and therapeutic resources are most constrained. These advances collectively point toward a future in which preeclampsia care moves from generalized risk scoring and reactive delivery toward precision medicine grounded in placental and immune biology. New therapies like metformin and DM199 may give us time; new molecular tools may finally tell us who needs it most.
References
- Cluver, C., et al. 2021. Use of metformin to prolong gestation in preterm pre-eclampsia: randomised, double blind, placebo controlled trial. BMJ.
- Cluver, C.A., et al. 2025. Safety and potential efficacy of DM199, a tissue kallikrein-1 analogue, for treating pre-eclampsia and fetal growth restriction: study protocol for a South African, hospital-based phase I/II open-label trial. BMJ Open.
- McElrath, T.F., et al. 2025. Utility of the US Preventive Services Task Force for Preeclampsia Risk Assessment and Aspirin Prophylaxis. JAMA Network Open.
- Elovitz, M.A., et al. 2025. Molecular subtyping of hypertensive disorders of pregnancy. Nature Communications.
- Zeisler, H., et al. 2016. Predictive Value of the sFlt-1:PlGF Ratio in Women with Suspected Preeclampsia. New England Journal of Medicine.
Further reading and resources
- Preeclampsia Foundation – patient education, advocacy, and research resources
- Preeclampsia Research – academic research collaboration
- DiaMedica Therapeutics — Preeclampsia pipeline – clinical development of DM199
- Mirvie – prenatal RNA-based diagnostics for preeclampsia and preterm birth
Summary and article by Stefan Botha



